Welcome to Dr. Arunava Lala
Welcome to Dr. Arunava Lala

The hand consists of 27 bones (including the 8 bones of the wrist). Intricate in design and function, the hand is an amazing work of anatomic engineering and is an amazingly multi functional and indispensable part of our body.
When the other associated structures (nerves, arteries, veins, muscles, tendons, ligaments, joint cartilage, and fingernails) are considered, the potential for a variety of injuries exists when trauma involves the hand. Therefore, any injury to the underlying structures of the hand carries the potential for serious handicap. To reduce this risk, even the smallest hand injuries require proper medical evaluation.
The goal of the treatment for injuries to the hand is a rapid and accurate initial evaluation and treatment. In other words, once an injury occurs, an experienced orthopedist such as Dr Arunava Lala strives to begin medical treatment quickly so the short- and long-term effects on the hand can be minimized.
• Thumb sprains
• Wrist sprains
• Injuries to the bone
• Hand fractures
• Wrist fractures
• Dislocations of the pip joint
• Soft tissue and closed tendon injuries
• Finger injuries
• Wrist injuries
• Broken hand
Hand Injury Symptoms
The symptoms of hand injuries can vary depending on the type of injury, how the injury occurred (mechanism), depth, severity, and location and are as follows :
• Tenderness (pain), Deformity, Swelling and discoloration, Bleeding, Numbness, Decrease range of motion (difficulty moving), Weakness, Decrease in range of motion.
• Anyone with a hand injury should consider calling a doctor or seek medical attention. The potential for devastating injuries increases greatly when medical attention is delayed. Even the smallest cut or seemingly innocent hand injury could require advanced treatment to prevent infection or significant loss of function.
Seek emergency medical care in these situations:
• Fractures, dislocations, high pressure injuries, and amputations require immediate care.
• Soft tissue injuries and amputations: Any deep, gaping (open), or dirty cut requires prompt medical care.
Dislocations
• Evaluation to determine extent of injury
• Pain relief
• X-ray to rule out fracture and further define injury
• Local anaesthesia
• If there is no fracture or associated laceration, reduction to put bone back in place is attempted; reduced reduction of bones is painful, so some patients will require pain medication for the procedure.
• Re-examination of the injury
• Immobilization by splinting or budding taping
• X-ray for confirmation of correct alignment
• Follow-up with hand surgeon or orthopedist, usually within 24-48 hours.
Dislocations are the result of injuries to the ligaments around joints. In a dislocation, a bone is displaced out of normal position resulting in obvious deformity, pain, and decreased mobility. When a dislocation occurs, the doctor will evaluate the injury to ensure there are no fractures. Dislocated bones must be put back in place. This process is called reduction, which is the realignment of dislocated or broken bones. Reduction can be accomplished by external manipulation of the injured area (closed reduction) or by surgery (open reduction). All require follow-up care after a period of immobilization, usually with a splint or cast. The goal of treatment is to preserve the function and stability of the joint.
Splinting describes any method used to keep the injured hand or finger from moving. The doctor may place an injured hand or finger against a solid, stiff object but not inside a cast. With a splint the injured area is immobilized yet still has room to swell. A cast does not allow for swelling, so the injury may be casted a few days after swelling has decreased.
Buddy taping is a procedure where the doctor tapes an injured finger to an adjacent finger to keep the injured finger from moving. The other finger becomes a splint.
Fractures (Broken Bone)
• Evaluation to determine extent of injury
• Pain relief
• X-ray
• Referral for operative repair or acute reduction; some patients will require conscious sedation (anaesthesia technique where the patient is not fully sedated, but does not require ventilation assistance).
• Referral for failed/inadequate reduction
• Re-examination
• Immobilization by splinting or budding taping
• X-ray for confirmation of correct alignment
• Follow-up with primary care doctor or hand specialist for severe or complicated fractures
Fractures of the hand and wrist are fairly common. Most fractures heal well if treated in a timely and appropriate manner. Some injuries may require a series of X-rays over one to two weeks. The small bones and complex structure of the hand make some fractures difficult to detect. The treatment of fractures depends on a number of factors including the severity of the crack or break, whether joints are involved, the location of the specific bone injured, the amount of deformity (displacement), and if there is a laceration (cut) associated with the fracture.
Children’s bones are still growing and so are susceptible to fractures involving the soft areas where the bone growth is actually occurring (growth plate). Some of these growth plate injuries are difficult to diagnose because they do not show up on X-rays. Injuries near the growth plate areas of a child’s hand therefore may need to be treated as fractures (breaks) even with normal X-rays. Some doctors will X-ray the opposite uninjured hand to compare with the injured hand to assist with visualizing growth plate fractures or disruptions.
Treatment of a recent fracture rarely includes an enclosed cast. Fractures and other injuries that require immobilization are often splinted on one side to prevent compression injuries from a cast that covers the entire hand. A splint allows room for the swelling associated with acute injuries, which may prevent the loss of adequate circulation or nerve injury. Splinting does not entirely eliminate the possibility of this complication. Anyone who experiences numbness, color change, or the feeling of tightness after splint application should return to the doctor immediately or go to the emergency department. Recovery time from a hand injury depends on the nature of the damage and the force of the impact.
3 months after a distal end of radius fixation!!!


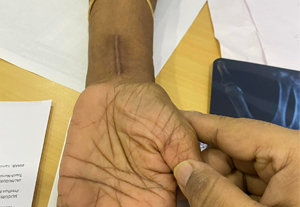
45 year old man with volar Barton type fracture….giving full range of motion in 3 months follow up!!


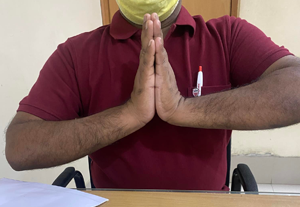
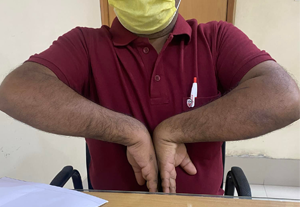
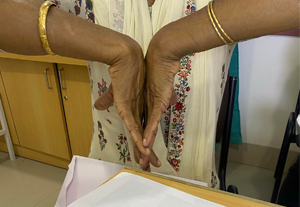
6 months follow up of a intra articular fracture of distal radius…..happy and satisfied patient!!






1yr old malunited distal end radius fracture…..presented with re-injury. Open reduction of distal radius and excision of distal ulna done. 75yr old gentleman came for his 3 month follow up. Pleasantly surprised with his grip strength, power and pain free range of motion.






Copyright © 2025 Dr. Arunava Lala. All Rights Reserved.
Website Designed & Developed by Web Hub Solution









